
Research Article | DOI: https://doi.org/10.31579/2693-2156/008
1 Cardiovascular Surgeon, Hospital Universitario San Ignacio. Assistant Professor, Faculty of Medicine, Pontificia Universidad Javeriana, Candidate for Clinical Epidemiology Magister, Carrera 7 #40-62 Bogotá, Colombia
2 Cardiovascular Surgeon, Head of the Cardiovascular Surgery Unit, Hospital Universitario San Ignacio, Pontificia Universidad Javeriana, Carrera 7 #40-62, Bogotá, Colombia.
3 Medical Student, Pontificia Universidad Javeriana, Carrera 7 #40-62, Bogotá, Colombia
4 Medical Student, Pontificia Universidad Javeriana, Carrera 7 #40-62 Bogotá, Colombia
5 Research Assistant, Clinical Epidemiology and Biostatistics Department, Faculty of Medicine, Pontificia Universidad Javeriana, Carrera 7 #40-62, Bogotá, Colombia
6 Associate Professor, Clinical Epidemiology and Biostatistics Department, Faculty of Medicine, Pontificia Universidad Javeriana, Carrera 7 #40-62, Bogotá, Colombia
*Corresponding Author: Giovanny Rios Dueñas, MD, Cardiovascular Surgeon, Hospital Universitario San Ignacio. Assistant Professor, Faculty of Medicine, Pontificia Universidad Javeriana, Candidate for Clinical Epidemiology Magister, Carrera 7 #40-62 Bogotá, Colombia.
Citation: Giovanny Rios-Dueñas, Juan Rafael Correa-Ortiz, Juliana Villanueva-Congote, Emilio Chala-Saad, Marian Rincon-Montaña, Camila Pantoja-Ruiz, Diego Rosselli, (2020) Non-Cardiac Thoracic Surgical and Endovascular Perioperative Major Adverse Cardiac Events: Quick and Easy Prediction and Proposed Mitigation Strategies. J Thoracic Disease and Cardiothoracic Surgery, 1(2); DOI:10.31579/2693-2156/008
Copyright: © 2020 Giovanny Rios, This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Received: 05 June 2020 | Accepted: 26 June 2020 | Published: 09 July 2020
Keywords: cardiac surgical procedures; open heart surgery; minimally invasive cardiovascular surgical procedures; costs and cost analysis
Background: The aim of this study was to describe the experience with minimally invasive cardiovascular surgery (MICS) by evaluating the costs and clinical outcomes in a university hospital in Bogotá, Colombia. As a comparison, a series of patients submitted to open heart surgery (OHS) was used.
Methods: Through a retrospective analysis of clinical records, from January 2014 to September 2018, data from 56 patients submitted to either MICS or OHS were collected. A comparison between these two types of approaches evaluating relevant clinical outcomes and demographic differences was performed. Direct costs for each hospitalization were analyzed and discriminated by categories. Costs are presented in 2018 US dollars (USD).
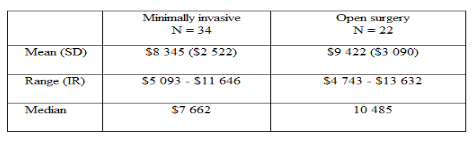
Results: Thirty-four patients were included in the MICS group, with ages ranging from 17 to 63 years; 22 patients were included in the OHS group, with ages from one to 74. The mean length of stay was 6.9 days (SD 3.4) in the MICS group and 10.3 (SD 6.5) in the OHS (p = 0.046). The average cost for MICS was $8 345 ± 2 522 and for OHS was $9 422 ± 3 090 (p=0.08). Higher costs in procedures in MICS where compensated by lower costs in hospital stay, laboratory tests, medications and transfusions.
Conclusion: MICS can be performed safely in a middle-income country like Colombia, at a fraction of the costs incurred in developed countries, while improving hospital bed turnover rate.
In 1952, the first open-heart surgery (OHS) was successfully performed in a 5-year-old girl for the reparation of an atrial septal defect. Previously, major vascular surgery was limited to extracardiac procedures, such as aortic coarctation repair or ductus arteriosus ligation. In 1953 Gibbon performed an atrial septum defect repair using a cardiopulmonary bypass system for 26 minutes but could not repeat this surgery successfully. Modern cardiac surgery had started [1,2]
The first minimally invasive cardiovascular surgery (MICS) took place in 1948 when Harken and Ellis described a mitral valvotomy using an intercostal approach [3]. In 1994, Benetti and Ballester, two Argentinean surgeons, described the anastomosis of the internal mammary artery with the anterior descending artery, through a small anterolateral thoracotomy [4]. Two years later, in the Cleveland Clinic, Cosgrove and Sabik described MICS for aortic valve replacement using a parasternal and transsternal incision, Carpentier performed the first video-assisted mitral repair, and Leipzig worked with the first three-dimensional videoscope in Germany [5]. MICS for correction of auricular septal defects has been reported with good clinical results, and low frequency of adverse events [6].
Despite being safe, MICS has disadvantages, related to the need for femoral cannulation, for ligation of the right internal mammary artery, thoracic instability and, in case of any complications, difficulty for conversion to a full sternotomy [7]. MICS should be understood as part of the trend towards less invasive and less traumatic procedures [8,9]. Appropriate surgical technique, proper selection of patients and an experienced surgeon should be associated with mortality close to 0%. In addition, these types of approaches leave less visible defects, which are the expected result for patients [4]
Advantages of MICS for mitral valve replacement were described by Carpentier in 1996. And have been proven in other studies [10]. Given the requirements of specialized equipment, longer surgical time [11], use of cardiopulmonary bypass and clamping times, this procedure has higher costs compared to OHS [7], despite decreasing both length of stay and need for blood transfusion [11]. One of the disadvantages of MICS for aortic valve replacement is limitation in visibility during the procedure, which can complicate cannulation, ventilation of the heart and placement of the epicardial wires. Despite this, it is less traumatic, improves ventilatory mechanisms, and reduces postoperative pain, infection rate, bleeding volume and transfusion requirements. All this allows patients to return to their daily activities sooner [12].
Cardiovascular surgery is expensive, according to Iribarne et al. direct costs for both MICS or OHS cost $20,000-30,000 USD [13]. The aim of this study was to describe the experience of MICS by evaluating costs and clinical outcomes in a cardiovascular surgery unit of a university hospital in Bogotá, Colombia. As a comparison, a series of patients submitted to OHS was used.
A retrospective analysis of the cardiovascular surgery database of the university hospital was conducted and the clinical data were collected from January 2014 to September 2018 since MICS was introduced in the hospital in 2014. Patients who underwent MICS were included, and patients operated for OHS were chosen for comparison.
Patients required some other additional cardiovascular procedure in the same period were excluded. Multiple parameters were compared between the two types of approaches, including evaluating the surgical times, the time stayed in the hospital and the intensive care unit (ICU), bleeding volume during surgery, blood transfusion requirement, intubation, or hemodynamic support; as well as the direct medical costs for each hospitalization. The costs were discriminated among procedures, medicines, laboratories, images and hospital stay.
GraphPad Prism 6 software was used for statistical analysis. The demographic differences, ICU and hospital stay, intra-surgical bleeding volume, time of surgery, cardiopulmonary bypass and clamping, and hemodynamic support requirement were initially analyzed by the D'Agostino-Pearson Normality Test. For the variables that did not pass the normality test, U Mann Whitney test was used. When the results were not statistically significant, median and interquartile ranges were reported.
All costs in Colombian pesos (COP) were adjusted from pesos of 2018 using the health price index (IPC) specifically estimated by the national statistics agency DANE. Afterward, costs were converted to US dollars (USD) with the official average exchange rate of the Central Bank of Colombia (Banco de la República) $1USD = $2956 COP. Then the Shapiro Wilk normality test was applied and the U Mann Whitney test with continuity correction if the normality test was not fulfilled.
This study complies with international and local ethical regulation and was approved by the University Hospital research and ethics committee.
Thirty-four patients were included in the MICS group, with ages ranging from 17 to 63 years; 22 patients were included in the OHS group, with ages from 1 to 74 (Table 1).
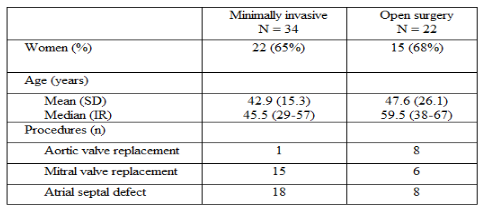
The proportion of females was similar in both groups, and although mean age was higher in the OHS, the difference was not statistically significant (p=0.06). Patients were mostly adults, but in the group of OHS, there were 5 children aged between 7 months and 9 years. Despite the 5 pediatric cases, the average age in the OHS group was 5 years higher than the MICS group. Atrial septum defect repair was the most common procedure, particularly in the MICS group, followed in frequency by mitral valve replacement. Only one aortic valve replacement was performed by MICS while 8 of these were performed by OHS. In the OHS group, the less common procedure was mitral valve replacement.
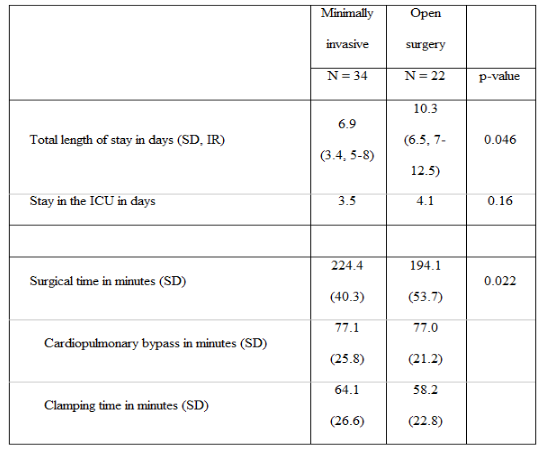
Although all patients were taken to the ICU in the postoperative period and required ventilation, 5 patients were admitted to the ICU with orotracheal intubation in the MICS group and 1 in the OHS group. However, 29 of the 34 MICS patients were extubated in the operating room, and only 3 required positive pressure ventilation. Of those from OHS, 21 out of 22 patients were extubated, but 11 needed positive pressure assistance after surgery. Table 2 summarizes data about length of stay and surgical times.
The need for hemodynamic support was similar, 10 patients required support in MICS and 10 in OHS (p = 0.262). Although there was no difference in the bleeding volume (mean 135 ±106 (cc) in MICS, 268 ±125 (cc) in OHS; p =0.12), there was a difference in the requirement for blood transfusion. In the MICS group, two patients required it (1 and 2 pRBC.), while in the OHS group 8 patients required transfusion (4 required 1 unit of pRBC, 3 required 2 and 1 required 3 units). Total costs are summarized in Table 3.
Shapiro Wilks normality test for the costs of the MICS group rejected the hypothesis of normality (p<0>Figure 1.

On the other hand, the OHS group did not have a statistically significant value for this same test (p=0.12). Mann Whitney test with continuity correction did not show a difference for the average costs in the MICS and OHS groups (p = 0.08).
Despite having similar costs, the analysis of cost components differs between both groups. The cost of medical supplies (excluding medication and blood components) were higher in the MICS group, representing 51.5% of total costs ($4 296 of the total of $8 345) than in the OHS group (38.3% of total cost; $3 608 of $9 422). There were reductions in the relative costs of medications (which represented 11.2% of total costs in MICS and 15.5% in OHS); length of stay (which represented 10.4% of total costs in MICS and 14.9% in OHS); laboratory tests (3.6% in MICS and 4.2% in OHS); and blood bank costs (1.2% in MICS and 4.0% in OHS).
This study has several limitations. The sample size is relatively small compared with those from large academic centers in the United States, which relates to the relatively recent implementation of MICS in a middle-income country like Colombia. Moreover, the comparisons of these two groups would have been more appropriate with a randomized allocation of study subjects. The OHS group was more heterogeneous in age, with young children and more elder subjects; surgical procedures in both groups are not necessarily comparable.
In our MICS group the most common procedure was the correction of the atrial septum defect, followed by mitral valve replacement, unlike other series, like the one described by Iribarne et al. [14] at the Columbia University Medical Center in New York, of 910 patients submitted to MICS, where mitral surgery predominates (507 patients) over correction of septal defects (103 patients). In our study all patients in the MICS group were adults (17 or older), while the OHS group included several children. The mean and median length of stay of our MICS sample were identical to this larger sample. Our mean clamping time (64.1 ± 26.6 m) was also similar to theirs (58.1 ± 44.9) but cardiopulmonary bypass was shorter in our patients (77.1 ± 25.8 m vs. 101.9 ± 66.8).
Another Indian study by Chigarapalli et al. [15] with a sample of 70 patients submitted to MICS, showed that the most common procedure was correction of atrial septal defect (30 patients), followed by mitral valve replacement (25 patients), similar to the findings in our study. This study did not include children, same as ours. The mean length of stay (6 days) reported in this study was identical to ours, but our ICU stay was a day longer. The mean clamping time and cardiopulmonary bypass were shorter for the patients in this study (26.16± 5.48 and 51.28± 11.13 m respectively).
As has been described elsewhere [13,14], MICS was associated with a shorter length of stay in our institution. This 3-day reduction is particularly significant in a hospital like ours, and very probably in most low and middle-income countries where hospital beds, operating rooms and ICU availability constitutes yet another access barrier to high complexity procedures [16]. Even if there were no savings for the health system with MICS, increasing bed availability would be an advantage by itself. Future studies, from the patient perspective, could analyze the influence on quality of life not only in the mid-term [17,18] but also in the immediate postoperative period, as has been suggested elsewhere [19–21].
With regard to costs, several findings are interesting when placed in the context of other similar studies. While in Colombia this high complexity procedure costs between $5 000 and $14 000 for 2018, in Columbia University Medical Center costs $20 000 to $30 000 for 2011 (9). The distribution of costs in our MICS group, with two peaks (Figure 1), one around $6 000 and the other around $11 000 was an unexpected finding and deserves further analysis. Despite ending up with similar costs in both groups, the component of these reflect an increase in procedural costs, compensated with a reduction related to shorter length of stay, medications, lab tests and blood bank costs.
In summary, MICS is a viable option in a middle-income country like Colombia, reaching similar clinical and safety outcomes as those described in more developed countries, at a fraction of the cost. Shorter length of stay could be an added advantage where hospital has limited available beds.
We thank Julie Johana Rojas Villamil for her assistance with data collection.
Dear Editorial Team, Clinical Medical Reviews and Reports. My experience with the journal was highly positive. The peer-review process was rigorous, constructive, and completed in a timely manner. The reviewers provided valuable comments that helped improve the quality and clarity of our manuscript. The editorial office was professional, responsive, and supportive throughout all stages of the publication process. Communication was clear and efficient, and any questions were addressed promptly. Overall, I found the journal to maintain high scientific standards and an excellent publication workflow. I would be pleased to consider submitting future work to this journal. Best wishes from, Elena Popa.

It was my pleasure to submit my testimonial concerning the Reviewer Board of our Scientific Journal “Brain and Neurological Disorders”. The Reviewers focused on some modifications and their contribution was helpful. The ladies of our Editorial Office were also supported my efforts. It was my honor to have such a co-operation and I am looking forward for more collaboration.

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Thank you for the speedy and efficient peer review process. I appreciate the fact that your peer reviewers do not take months to respond like with some other journals. I would also like to thank the editorial office for responding quickly to my questions. It is an excellent journal. I plan to submit more manuscripts in the future. Best wishes from, Robert W. McGee

Dear Grace Pierce, Editorial Coordinator of Journal of Clinical Research and Reports, Working with you and your team on our recent publication in JCRR has been a truly wonderful and enjoyable experience. The responses were prompt, and the reviewers were patient, constructive, and highly professional. One reviewer in particular gave me the feeling that a professor was carefully reading and commenting on my coursework, which was deeply touching. The entire process was straightforward and hassle‑free, with no tedious online forms to complete. I highly recommend this journal. Best wishes from, DR Aibing Rao, Head of R&D

I Appreciate the Opportunity to Share my Experience with the Journal of Clinical Research and Reports. The peer review process was timely and constructive, and the feedback provided helped improve the quality of our manuscript. The editorial office was professional, responsive, and supportive throughout the process, ensuring smooth communication and efficient handling of the submission. Overall, it was a positive experience collaborating with your team.

Dear Mercy Grace, Editorial Coordinator of Obstetrics Gynecology and Reproductive Sciences, We would like to express our gratitude for your help at all stages of publishing and editing the article. The editors of the magazine answer all the necessary questions and help at every stage. We will definitely continue to cooperate and publish other works in the Obstetrics Gynecology and Reproductive Sciences! Best wishes from, Alla Konstantinovna Politova,
